

Patient Eligibility & Triggers
for Hospice Care
Palmetto GBA Local Coverage Determination

Amyotrophic Lateral Sclerosis (ALS)
Patients will be considered to be in the terminal stage of ALS (life expectancy of six months or less) if they meet the following criteria.
- Patients should demonstrate critically impaired breathing capacity.
- Dysphasia
- Wheelchair or bed-bound status
- Needs assistance in most or all (ADLs)

Alzheimer's Disease
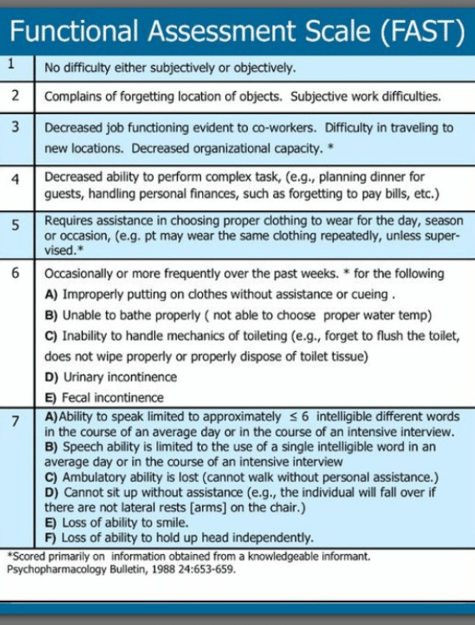
The FAST scale is a 16-item scale designed to parallel the progressive activity limitations associated with AD. Stage 7 identifies the threshold of activity limitation that would support a 6-month prognosis.
Stage 7: Loss of speech, locomotion, and consciousness:
7a: Ability to speak limited (1 to 5 words a day)
7b: All intelligible vocabulary lost.
7c: Non-ambulatory
7d: Unable to sit up independently.
7e: Unable to smile.
7f: Unable to hold head up.
The FAST scale does not address the impact of comorbid and secondary conditions.
Secondary conditions that are often related to and/or complicate Alzheimer's:
- Recent Falls
- UTI's
- Infections
- Pressure Ulcers
- Weight Loss
- Delirium
Structural/functional impairments and relevant activity limitations:
- Ambulation
- Continence
- Transfer
- Dressing
- Eating
- Bathing

Cancer
Medicare requires "clinical information and other documentation" to support the certification of individuals having a terminal illness with a life expectancy of 6 months or less if the disease runs its normal course.
There are many types of cancer; the following hospice cancer criteria are general rules physicians can use to determine if hospice is the right choice for a patient.
Clinical hospice cancer criteria may include the following:
- Metastatic cancer
- Decline in the condition despite therapy
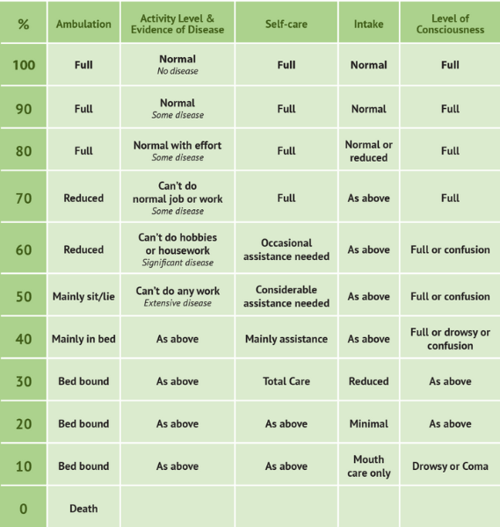
- Palliative Performance Score of 70% or less
- Electing to forgo further disease-directed curative treatment. (Palliative radiation or chemotherapy may still be included.)
Specific cancer diagnoses are often eligible for hospice without other criteria, including small cell lung cancer, pancreatic cancer, and primary CNS malignancy.
The Palliative Performance Scale is used to assess the progressive decline of palliative patients and is frequently used to determine if a cancer patient is eligible for hospice.

Cardiac/Heart Disease
Medicare requires "clinical information and other documentation" to support the certification of individuals having a terminal illness with a life expectancy of 6 months or less if the disease runs its normal course.
The International Classification of Functioning includes the following domains (Ranking No, Mild, Moderate, Severe, Complete Impairment):
- Structures of Cardiovascular & Respiratory Systems
- Functions of Cardiovascular & Respiratory Systems
- Communication
- Mobility
- Self-care
Identification of specific structural/ functional impairments and relevant activity limitations:
- Heart Valve Stenosis
- Ambulation
- Class IV NYHA
- Incontinence
- Difficulty with Transfers
- Severely reduced Ejection Fraction
- Impaired Self-care
- Abnormal Lab Values
- Abnormal oxygen saturation
- Irregular lung sounds
These impairments contribute to the increased incidence of secondary conditions, such as:
- Delirium
- Pneumonia
- Stasis Ulcers
- Pressure ulcers
- Falls
- Weight Loss
- Oxygen Dependence
- Other Infections
SPECIFIC DATA TO SUPPORT A HOSPICE DIAGNOSIS OF CHF:
- Identification of specific structural/functional impairments
- Ejection fraction <20% (not required, but an important consideration)
- A poor response to diuretics and vasodilators
- Dyspnea or tightness in the chest despite tx.
- Chest pain
- Impaired heart rhythms, contraction force of ventricular muscles, and impaired blood supply to the heart
- Changes in appetite, unintentional weight loss
- Impaired sleep functions
- Decline in general physical endurance
- Relevant activity limitations and or impaired mobility
If you are seeing any of the above signs and symptoms in a patient with CHF or end-stage cardiac conditions, it may be time to consider adding the support of hospice care.
SPECIFIC DATA TO SUPPORT A HOSPICE DIAGNOSIS OF COPD:
- Recent visits to the ER or hospitalization for pulmonary infections or respiratory failure
- Dyspnea or tightness in the chest (FEV1 <30% of predicted)
- Identification of specific structural/functional impairments
- Relevant activity limitations
- Changes in appetite and unintentional progressive weight loss
- Impaired sleep functions
- Decline in general physical endurance
- Impaired mobility
- Requires oxygen most, if not all, of the time
- May require breathing treatments or the use of inhalers
- May have difficulty eating or carrying on conversations without becoming short of breath.

End-Stage Renal Disease
End-stage renal disease (ESRD) may support a prognosis of six months or less under many clinical scenarios.
Documenting structural/functional impairments and activity limitations facilitates the selection of intervention strategies (palliative vs. long-term disease management/curative). It provides objective criteria for determining the effects of such interventions.
- Creatinine clearance of <10cc/min (<15cc/min for diabetics) AND serum creatinine >8.0 mg/di (>6.0mg/di for diabetics)
- Uremia with obtundation
- Nausea/Vomiting
- Patient has chosen not to have renal dialysis
- Intractable hyperkalemia
- Hepatorenal syndrome
- Structural and functional impairments
- Platelet count <25,000
- Comorbid and secondary conditions contribute to terminal prognosis
- Pruritus
- Self-care deficits
- Activity limitations
- Uremic pericarditis
- Anorexia
- Albumin < 2.5 gm/di

HIV/AIDS
Human Immunodeficiency Virus (HIV) Disease (1 and 2 must be present; factors from 3 will add supporting documentation)
1. CD4 + Count 100,000 copies/ml, plus 1 of the following:
- CNS lymphoma
- Untreated or not responsive to treatment, wasting (loss of 33% lean body mass)
- Mycobacterium avium complex (MAC) bacteremia, untreated, unresponsive to, or refused treatment.
- Progressive multifocal leukoencephalopathy
- Systemic lymphoma, with advanced HIV disease and partial response to chemotherapy
- Visceral Kaposi's sarcoma & unresponsive to therapy
- Renal failure in the absence of dialysis
- Cryptosporidium infection
- Toxoplasmosis, unresponsive to therapy
2. Decreased performance status as measured by the Palliative Performance Scale (PPS).
3. Documentation of the following factors will support eligibility for hospice care:
- Chronic persistent diarrhea for one year
- Persistent serum albumin < 2.5
- Concomitant, active substance abuse
- Age > 50 years
- Absence of antiretroviral, chemotherapeutic, and prophylactic drug therapy related specifically to HIV disease.
- Advanced AIDS dementia complex
- Toxoplasmosis
- CHF symptomatic at rest

Liver Disease
Patients will be considered to be in the terminal stage of liver disease if they meet the following criteria (1 and 2 must be present factors from 3 will lend supporting documentation):
- The patient should show both a and b:
- Prothrombin time prolonged more than 5 seconds over control or International Normalized Ratio (INR) > 1.5
- Serum albumin < 2.5 gm/di
- End-stage liver disease is present, and the patient shows at least one of the following:
- Ascites, refractory to treatment, or patient noncompliance
- Spontaneous bacterial peritonitis
- Hepatorenal syndrome (elevated creatinine and blood urea nitrogen (BUN) with oliguria (<400 ml/day) urine sodium concentration <10 mEq/I)
- Hepatic encephalopathy, refractory to treatment, or patient non-compliance
- Recurrent variceal bleeding despite intensive therapy
- Documentation of the following factors will support eligibility for hospice care:
- Progressive malnutrition
- Muscle wasting with reduced strength and endurance
- Continued active alcoholism (> 80 gm ethanol/day)
- Hepatocellular carcinoma
- Hepatitis B virus surface antigen (HBsAg) positivity
- Hepatitis C is refractory to interferon treatment.
- Patients awaiting liver transplants who otherwise fit the above
Criteria may be certified for the Medicare hospice benefit, but the patient must be discharged from hospice if a donor organ is procured.
SPECIFIC DATA TO SUPPORT HOSPICE DIAGNOSIS OF LIVER DISEASE
- Weakness and compromised ability to perform activities of daily living (ADLs)
- Recurrent variceal hemorrhage
- Hepatic encephalopathy
- Prothrombin time prolonged more than five seconds over control or INR > 1.5
- Serum Albumin < 2.5 gm/di
- Peritonitis
- Elevated creatinine and BUN with Oliguria <400 ml/day and urine Na concentration <10 mEq/I
- Ascites
- Malnutrition
- Muscle wasting
- Asterixis
- May be awaiting a liver transplant but would be discharged if a donor is procured.


Stroke
Regardless of the specific diagnosis, patients with neurological diseases are eligible for hospice services when they experience a continuous decline in functional or clinical status over time, leading to a poor prognosis with a life expectancy of six months or less if they meet the following criteria:
- Karnofsky Performance Status (KPS) or Palliative Performance Scale (PPS)
of 40% or less - Inability to maintain hydration and caloric intake with one of the following:
- Weight loss > 10% in the last six months or > 7.5% in the last three months
- Serum albumin < 2.5 gm/dl
- Current history of pulmonary aspiration
- Not responsive to speech-language pathology intervention
- Sequential calorie counts documenting inadequate caloric/fluid intake.
- Dysphagia severe enough to prevent the patient from receiving food and fluids necessary to sustain life in a patient who declines or does not receive artificial nutrition and hydration.

New York Heart Association (NYHA) Classification of Severity Heart Failure
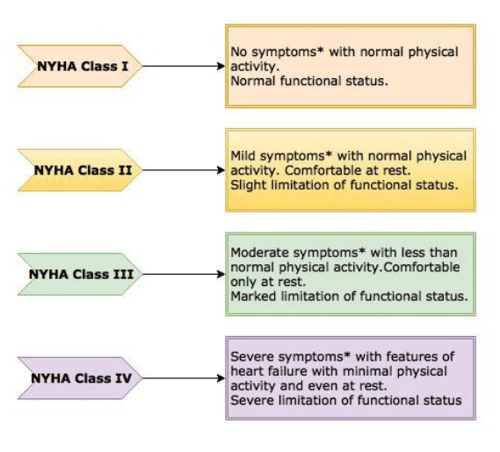
| Class I (mild) | No limitation on physical activity. Ordinary physical activity does not cause undue fatigue, palpitation, or dyspnea (shortness of breath) |
| Class II (mild) | Slight limitation of physical activity. Comfortable at rest, but ordinary physical activity results in fatigue, palpitation, or dyspnoea |
| Class III (moderate) | Marked limitation of physical activity. Comfortable at rest, but less than ordinary activity causes fatigue, palpitation, or dyspnoea |
| Class IV (severe) | Unable to carry out any physical activity without discomfort. Symptoms of cardiac insufficiency at rest. If any physical activity is undertaken, discomfort is increased |
Let HOPE Add Life To Your Days
Is it time for Hospice Care?
Still, have questions about whether a patient is eligible for hospice care? Contact HOPE Healthcare and Hospice for more information.
